

 KD HOLMES, LPC, EMDR CERTIFIED, BTTI TRAINED
KD HOLMES, LPC, EMDR CERTIFIED, BTTI TRAINED
OCD vs. Anxiety Disorders: Key Differences for Therapists
For therapists, understanding what is OCD for therapists-including the nuanced distinctions between OCD and other anxiety disorders-is essential for...
There is a moment in complex OCD treatment that every ERP therapist eventually meets. The client understands the model. They can explain the OCD cycle beautifully. They know reassurance does not help long-term. They can name their compulsions, identify their triggers, and even agree that avoidance is shrinking their life.
And still, the work does not move. Homework does not happen. Exposures get softened until they no longer touch the fear. Family members continue answering the same questions in increasingly creative ways. Sessions become long discussions about whether the client is ready, whether the exposure is ethical, whether the thought is “really OCD,” whether this one situation is different.
And somewhere in the room, quietly but powerfully, OCD starts running the meeting. This is where complex OCD treatment begins. Not because the client is “resistant.” Not because the therapist is doing it wrong. Not because the case is hopeless. But because ERP has moved from the clean lines of theory into the messy, human terrain of real clinical work.
Complex OCD treatment is not just harder exposures. It is better formulation.
When exposure and response prevention gets stuck, the first question is not, “How do we make this exposure more intense?” The better question is:
OCD is maintained by negative reinforcement. A trigger shows up. The client experiences distress, doubt, disgust, shame, uncertainty, or a sense that something is not right. Then comes the compulsion or avoidance behavior. For a moment, relief arrives. The nervous system exhales. The client feels safer, clearer, cleaner, more certain, or less responsible.
And OCD learns.
It learns that the ritual worked. It learns that uncertainty was dangerous. It learns that distress had to be escaped. It learns that the therapist, family, client, or environment can be recruited into the loop. In simple cases, the maintaining behavior may be obvious: washing, checking, repeating, avoiding, confessing, or reassurance seeking.
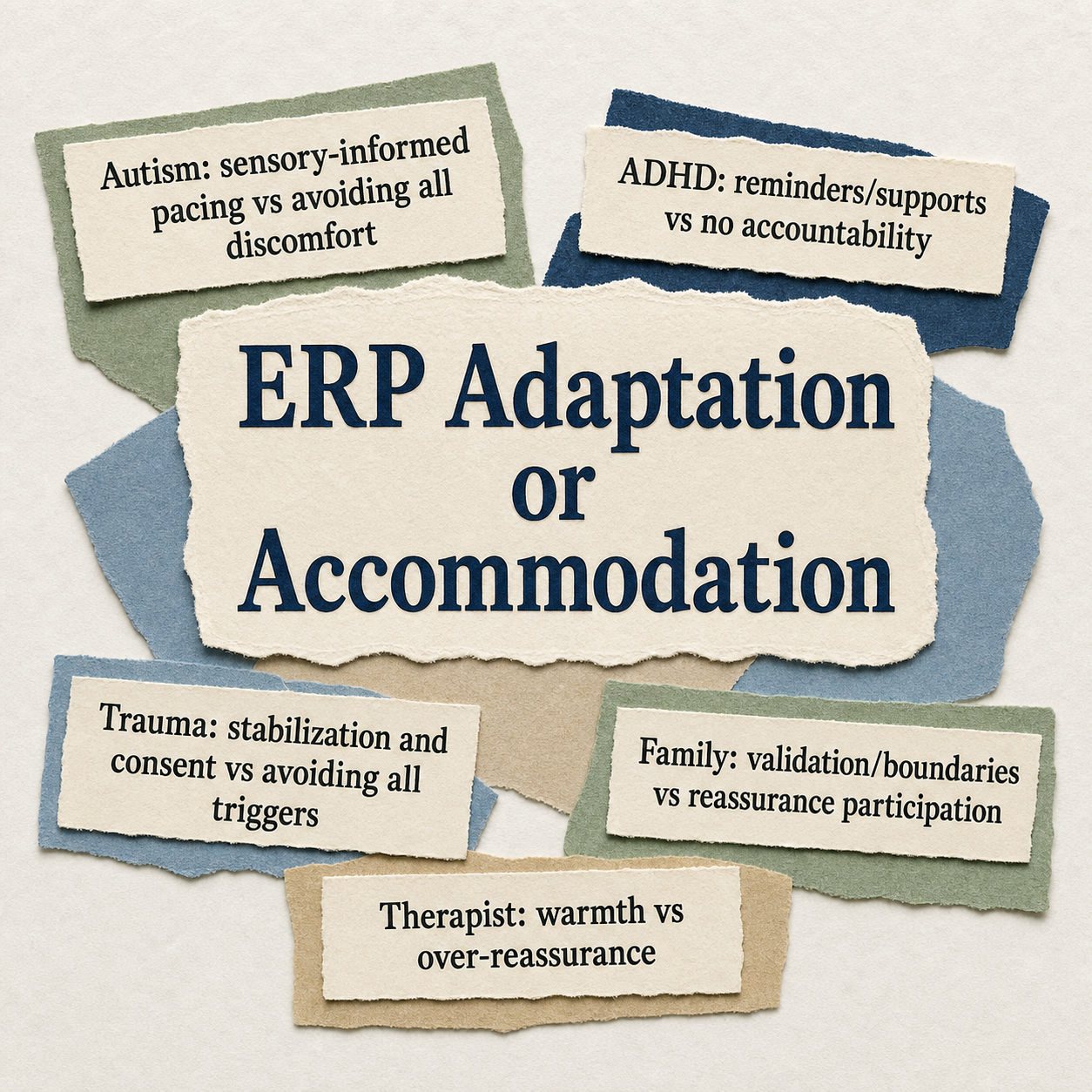
In complex OCD cases, the maintaining behavior often hides inside reasonable-looking clinical concerns. The client may need accommodations. The family may need education. Trauma may need careful pacing. ADHD may require executive-function supports. Autism may require sensory-informed planning. Depression may reduce capacity. Cultural context may shape what feels safe, moral, or possible. All of that matters.
But here is the fine line: adaptation should increase access to ERP. Accommodation protects OCD from being challenged. That distinction is everything.
Good ERP adaptation makes treatment more possible. It asks, “What does this client need in order to participate in response prevention?”
For a client with ADHD, adaptation might mean shorter exposure practices, visual reminders, timers, body doubling, or a simple homework plan that does not rely entirely on working memory.
For an autistic client, adaptation might include sensory-considerate environments, clear expectations, concrete language, predictable session structure, or distinguishing between a genuine sensory need and an OCD ritual.
For a client with trauma history, adaptation might involve consent, pacing, grounding, stabilization, and careful differentiation between trauma cues and obsessional predictions.
For a client with high shame, adaptation might mean more warmth, more normalization, and more time spent building a treatment frame that does not make them feel monstrous.
These are not watered-down ERP. These are access points. Adaptation says: “Let’s make the work possible.” Accommodation says: “Let’s make sure you do not have to feel the thing OCD says you cannot feel.” That is the difference.
Accommodation is tricky because it often looks compassionate. A parent answers “just one more” reassurance question because their child is sobbing. A partner changes routines because the household needs peace. A therapist avoids a taboo exposure because the client is already ashamed. A clinician spends half the session proving the obsession false because it feels cruel not to respond.
Nobody is trying to feed OCD. And yet, OCD is fed.
Family accommodation in OCD can look like reassurance, ritual participation, modifying routines, avoiding triggers, changing language, removing objects, helping the client check, or taking responsibility for things OCD has declared dangerous.
Therapist accommodation can be even more subtle. It can look like over-explaining. Over-reassuring. Avoiding direct exposure work. Letting every session become preparation for ERP rather than ERP. Debating obsessional content. Treating every spike in distress as a sign that something has gone wrong.
Sometimes therapist accommodation comes from our best qualities. We are empathic. We are careful. We do not want to harm. We know trauma exists. We know culture matters. We know clients have histories of being misunderstood. But OCD can use even our kindness if we are not paying attention.
The clinical question becomes: Am I supporting the client’s access to ERP, or am I helping OCD avoid uncertainty? Oof. Annoying question. Necessary question.
When ERP is stuck, it helps to name treatment-interfering behaviors without shame. Treatment-interfering behaviors are not character flaws. They are behaviors that block the work from happening.
They may include missed homework, repeated reassurance seeking, crisis escalation before exposure, refusal to track rituals, intellectualizing, switching themes when ERP gets close, canceling sessions after hard work, using skills to neutralize feelings, or turning every exposure into a negotiation with OCD.
Therapists can have treatment-interfering behaviors too. We may underdose ERP. We may avoid taboo topics. We may over-focus on insight. We may become too fascinated by content and lose the function. We may let sessions drift into supportive therapy because the exposure feels too sharp.
Again, this is not about blame. It is about seeing the room clearly. When we can name the interference, we can formulate it. What is the behavior doing?
Is it reducing distress? Avoiding shame? Preventing uncertainty? Protecting the therapist from fear? Keeping the family system regulated? Preserving the client’s identity? Avoiding rupture? Once we understand the function, we can choose the next intervention with more precision.
Complex OCD often involves more than one clinical process. OCD and PTSD can overlap. OCD and autism can overlap. OCD and ADHD can overlap. OCD can show up alongside depression, panic, dissociation, substance use, personality traits, family conflict, medical anxiety, or religious trauma.
This is where therapists can get tangled. If the client dissociates during exposure, we may need stabilization and pacing. If the client cannot initiate homework because of ADHD, we may need scaffolding. If the client is autistic and overwhelmed by sensory input, we may need to reduce unnecessary sensory load. If the client’s family is participating in rituals, we may need family work.
If the therapist is afraid of harm-related or taboo obsessions, we may need consultation. But none of those adaptations automatically mean we stop treating OCD. The question is not, “Is there comorbidity?”
The question is, “What is the function of this behavior right now?” A sensory support that helps an autistic client stay engaged may be clinically appropriate. A sensory rule that must be performed to prevent a feared consequence may be a compulsion.
Grounding that helps a trauma survivor remain oriented during ERP may be appropriate. Grounding used to erase uncertainty or neutralize obsessional distress may become a ritual. A reminder system for ADHD may support ERP. A tracking system that becomes perfectionistic certainty-seeking may become part of OCD.
Complexity does not remove the need for response prevention. It makes response prevention more specific.
One of the most under-discussed barriers in complex OCD treatment is therapist avoidance. We ask clients to approach what scares them. But therapists also have fear.
We fear increasing distress. We fear getting it wrong. We fear liability. We fear being misunderstood. We fear that harm-related thoughts mean something more dangerous. We fear sexual obsessions, religious obsessions, suicidal obsessions, aggressive images, identity fears, and family conflict.
So we soften. We talk around the exposure. We ask more assessment questions than needed. We reassure. We delay. We tell ourselves the client is not ready, when sometimes we are the ones not ready. To be clear: caution is not the enemy. Ethical care matters. Risk assessment matters. Consent matters. Cultural humility matters. Trauma-informed pacing matters. But avoidance dressed as caution can still become avoidance.
What would I do next if I trusted the formulation? Not if I ignored risk. Not if I bulldozed the client. Not if I performed ERP like a robot with a clipboard. If I trusted the formulation, what would be the next clinically honest step?
That question often brings the room back into focus.
Does this help the client approach the feared cue, prediction, sensation, uncertainty, or valued action?
Or does it help the client avoid distress, doubt, responsibility, disgust, shame, or uncertainty?
Does this support response prevention? Or does it make the compulsion more comfortable?
Does this increase flexibility? Or does it create another rule OCD can enforce?
Does this help the client return to life? Or does it make life smaller but calmer?
The goal of complex OCD treatment is not to make ERP harsher. It is to make ERP more accurate.
Sometimes that means slowing down. Sometimes it means involving family. Sometimes it means coordinating medication management. Sometimes it means treating depression or trauma more directly. Sometimes it means consulting. Sometimes it means making the exposure smaller, clearer, or more values-based.
And sometimes it means lovingly refusing to participate in the loop. That refusal can be deeply compassionate.
The art of advanced ERP is not being fearless. It is being willing.
Willing to assess carefully.
Willing to formulate honestly.
Willing to adapt thoughtfully.
Willing to stop reassuring.
Willing to notice when we, the therapists, have become part of the cycle.
Willing to help clients carry uncertainty without abandoning them inside it.
Complex OCD cases ask more of us. They ask us to understand comorbidity without losing the OCD. They ask us to honor trauma without making avoidance the treatment plan. They ask us to affirm neurodivergence without reinforcing rituals. They ask us to validate suffering without validating OCD’s demand for certainty.
That is not easy work. But it is good work. And when ERP gets stuck, the stuckness is not the end of treatment. It is information. It is the case saying: look closer.
What is maintaining the loop?
What is being avoided?
Who has been recruited into the ritual?
What support is actually needed?
What adaptation would increase access?
What accommodation needs to gently stop?
That is where complex OCD treatment begins. And that is exactly the kind of clinical work that turns ERP from a protocol into a craft.


For therapists, understanding what is OCD for therapists-including the nuanced distinctions between OCD and other anxiety disorders-is essential for...

There’s a particular kind of quiet that settles over the room when a client understands Exposure and Response Prevention Therapy and agrees to an...

Obsessive-Compulsive Disorder (OCD) is characterized by persistent, unwanted obsessions and repetitive compulsions. For an obsessive compulsive...