

 Whitney Storey, MS, LPC, ASDCS
Whitney Storey, MS, LPC, ASDCS
1 min read
Autism, Addiction, and Disordered Eating (OH MY!)
If you are a therapist offering Autism Therapy for a adults its important to consider disordered eating and addiciton. When consulting with mental...
-1.png)
Mental health professionals are trained in a way that leads us to spot the "obvious" cases of autism: the children who struggle with eye contact, who have high support needs, or who exhibit the classic externalized behaviors we learned in the media, our textbooks, and the DSM. But what happens when the signs aren't obvious? What happens when our clients are bright, articulate, and "successful," yet they keep appearing in our offices for treatment-resistant anxiety, chronic burnout, and a lifelong feeling of being an alien in their own lives? What are the signs of Autism in an Adult?
In many of these cases, we aren't seeing a failure of therapy (on the client's part or ours): we are seeing the result of missed diagnosis. For an entire generation, especially women, people who are gender and/or sexual minorities, and high-masking men, autism was never considered as an explanation of their difficulties because it didn't look like the 90s stereotype.
Being an effective clinician in today's world means keeping on top of the most recent neurobiological research and the lived experiences of late-diagnosed Autistic people and embracing neurodiversity-affirming care. Transitioning to a neurodiversity-affirming practice means learning to look through the "mask" to see the autistic nervous system underneath.
One of the most pervasive misconceptions in our field is that autism is a disorder of childhood. As defined in the DSM-5-TR, autism is a neurodevelopmental disorder that is present in the early developmental period (American Psychiatric Association [APA], 2022), but it doesn't disappear at the age of 18.
Instead, the "observable" traits simply become more internalized. Many adults who were missed as children developed what we call compensatory strategies. They studied their peers like social scientists, memorized scripts, and forced themselves to endure sensory environments that were physically painful.
To the outside world, they are "flying under the radar." But as clinicians, we must ask: At what cost? When a client presents with what looks like "Social Anxiety," but describes the experience as an intellectual decoding process rather than an emotional fear, we should be thinking about autism.
The most common reason a late-identified autistic adult finally seeks therapy is not for an autism diagnosis. They seek help because they have hit a wall of Autistic Burnout.
In my practice, I often see this mislabeled as Major Depressive Disorder. While they share surface-level symptoms like fatigue and withdrawal, the underlying mechanism is different. Autistic burnout is the result of years (and in my office, often decades) of "masking" and trying to live by neurotypical standards. It is a state of total nervous system depletion.
If we treat burnout with traditional "behavioral activation" (pushing the client to search for a different job or to get out more and socialize), we may actually be causing further harm. What an autistic brain in burnout needs is radical demand reduction and sensory regulation, not more social exposure.
Historically, the clinical world framed autism through the lens of Theory of Mind (ToM), which is the cognitive ability to "read" and understand others’ mental states. The prevailing narrative has been that autistic people have a fundamental "deficit" in this area, implying they were incapable of understanding that other people have different thoughts, feelings, or intentions, but that these empathy skills were capable of being taught and learned.
This is where the disconnect begins. If autistic and allistic (or not autistic) people struggle in their communication with one anothr, the assumption has always been that the autistic person has a communication deficit, with their "broken" ToM as the culprit.
Damian Milton’s theory of the Double Empathy Problem suggests that communication breakdowns between autistic and neurotypical people are a "two-way street." It isn't that the autistic person lacks empathy; it's that two people with different neurotypes are essentially speaking different "neurological languages." Communication issues are not a result of one person's deficits, but rather a reflection of struggles between both of the parties in the conversation.
Source: Milton (2012): On the Ontological Status of Autism: The ‘Double Empathy’ Problem
When we see a client who doesn't use standard eye contact or who speaks in a "monotone" or "blunt" way, our neurotypical bias may label them as "unengaged" or "cold." However, research shows that autistic people communicate quite effectively with other autistic people. The "deficit" only appears when they are forced to bridge the gap to a neurotypical standard. As clinicians, the burden of bridge-building should be on us.
The current autism diagnostic gap is most pronounced in individuals assigned female at birth (AFAB). For decades, the diagnostic criteria were based almost exclusively on the "Little Professor" male stereotype, which is at least partially the result of decades of research on young, middle-class white boys - almost exclusively. Our academic and clinical understanding of autism is based on such a specific group, it led to the research and DSM criteria for autism being a reflection of that limited group. The very way we understand and identify autism is limited to that same specific group. For example, even as recently as the 90s and early 2000s, Simon Baron-Cohen, a prominent autism researcher from Cambridge University, has referred to Autism as an "Extreme Male Brain".
Source: Baron-Cohen (2002): The Extreme Male Brain Theory of Autism
Research indicates that AFAB autistic people often have an "internalized" phenotype. Their intense interests may be more socially acceptable (e.g., psychology, art, or animals), and they are often socialized to be more "agreeable," which drives them to become master "maskers" from a very young age. Many AFAB autistic people focus on people in general, or communication a special interests, causing them to become highly skilled at people-ing, which prevents them from being identified as autistic early in life.
Source: Bargiela et al. (2016): The Experiences of Late-Diagnosed Women with Autism
Many of these clients are misdiagnosed with Borderline Personality Disorder (BPD) because of their difficulty with forming and maintaining friendships, their sensory meltdowns are misinterpreted as emotional instability, or their deep need for routine is seen as "controlling" behavior. It is not uncommon for AFAB autistic people to discover their own neurodivergence, especially in the world of the TikTok algorithm, before their family members and/or helping professionals in their lives.
In traditional therapy, we are trained to prioritize Top-Down processing. This is an information processing style based on a "concept-first" approach: the brain uses prior knowledge, expectations, and social labels to filter and categorize the world. You see a "cluttered room," and your brain instantly summarizes the scene so you can focus on the person sitting in front of you. You ignore the hum of the fridge because your "Top-Down" filter has labeled it as irrelevant.
However, for many autistic individuals, the brain operates primarily through Bottom-Up processing.
In a Bottom-Up system, the brain doesn't start with the "big picture" or a pre-existing label. Instead, it takes in every single data point—every sound, every flicker of light,ทุก scent—as a unique and intense piece of information.
When we focus purely on "Top-Down" cognitive behavioral shifts, like challenging a "distorted thought," we might be ignoring the fact that the client’s "Bottom-Up" foundation is currently under siege.
Autism involves a significant difference in how the brain filters this raw data. A flickering fluorescent light or the hum of an air conditioner in your office isn't just "background noise" that they are over-focusing on; it is a raw, unfiltered sensory input that their brain hasn't deprioritized. To an autistic client, that hum can be as intrusive and painful as a physical alarm.
Source: Robertson & Simmons (2013): The Relationship Between Sensory Sensitivity and Autistic Traits
When we understand that an autistic brain is processing the world from the bottom-up, our clinical lens shifts. When a client becomes "fidgety," avoids eye contact, or suddenly shuts down during a breakthrough moment, we can no longer default to labeling it a "psychological defense" or "resistance."
In many cases, it isn't a cognitive avoidance of the topic—it’s a sensory overload triggered by the environment.
A neurodiversity-affirming practice recognizes that if the "bottom-up" foundation is unstable, the "top-down" therapeutic work cannot happen. Creating a safe space starts with the physical environment and explicit communication:
We don't ask the client to adapt to our office; we adapt the office to the client’s nervous system. This shifted focus then becomes the foundation for how we encourage our clients to relate to the world outside of the therapy room as well.
For decades, the unspoken metric for "success" in autism therapy was how well a client could blend in. If they stopped flapping their hands or an learned to script small talk, the intervention was labeled a victory. Many family members and autistic people themselves will seek help for "social skills," usually meaning that they want to learn to be more "normal."
However, we know that training someone to suppress their natural impulses, which is what we mean by the process of "masking," is not a "social skill." It is a constant, high-stakes performance that consumes immense cognitive energy and contributes in significant ways to Autistic burnout.
When the goal of therapy is to make an autistic person "appear more neurotypical," we aren't providing healthcare; we are practicing a form of conversion therapy. We prioritize the comfort of the allistic observer over the well-being of the autistic individual. Truly neurodiversity-affirming therapy will, instead, :
Source: Gaddy & Crow (2023): A Primer on Neurodiversity-Affirming Services
When an adult receives an autism diagnosis at 30, 40, or 60, they don't just get a label. They get a new lens for their entire life history. They begin to realize that their "social failures" were actually communication mismatches, and their "laziness" was actually sensory exhaustion. It can be a deeply emotional shift, with positive and negative consequences for every part of their lives.
As clinicians, we have the power to be the person who finally "sees" them. By moving beyond outdated stereotypes and embracing a neurodiversity-affirming framework, we can help our clients stop surviving a world that wasn't built for them and start building a life that honors who they actually are.


1 min read
If you are a therapist offering Autism Therapy for a adults its important to consider disordered eating and addiciton. When consulting with mental...
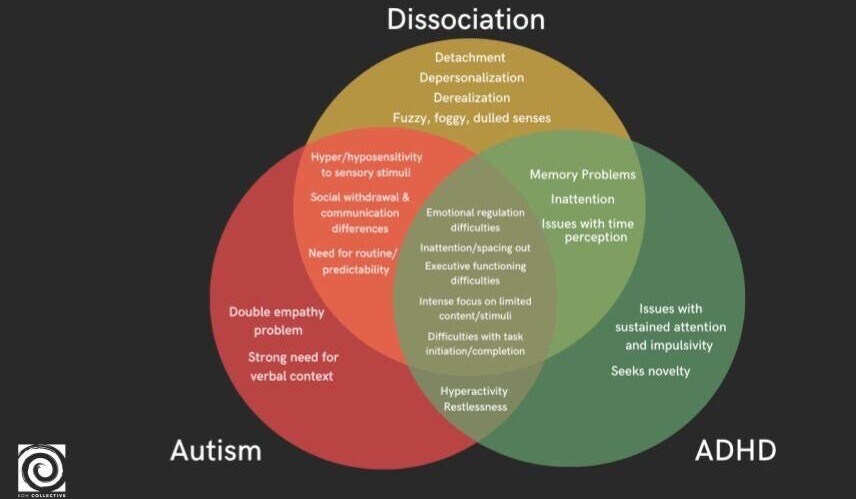
Exploring the complexities of mental health, the threads of neurodivergence and dissociation weave together in intricate patterns. For therapists,...
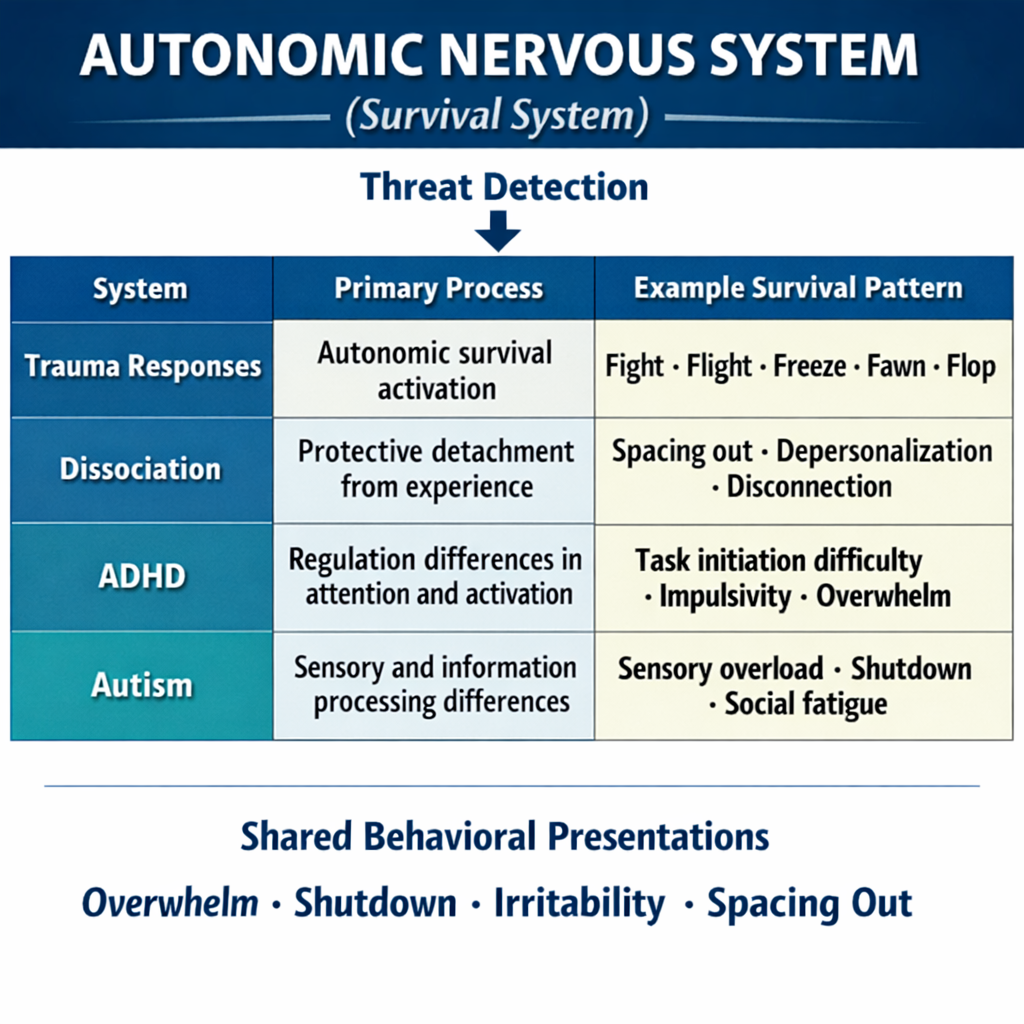
Most therapists today are familiar with the language of the nervous system. Fight, flight, freeze, fawn, and flop have become central to...