

 KD HOLMES, LPC, EMDR CERTIFIED, BTTI TRAINED
KD HOLMES, LPC, EMDR CERTIFIED, BTTI TRAINED
Navigating Neurodivergence Trauma
For therapists, trauma-informed care is a primary focus in both training and treatment. This approach, characterized by sensitivity to trauma and its...
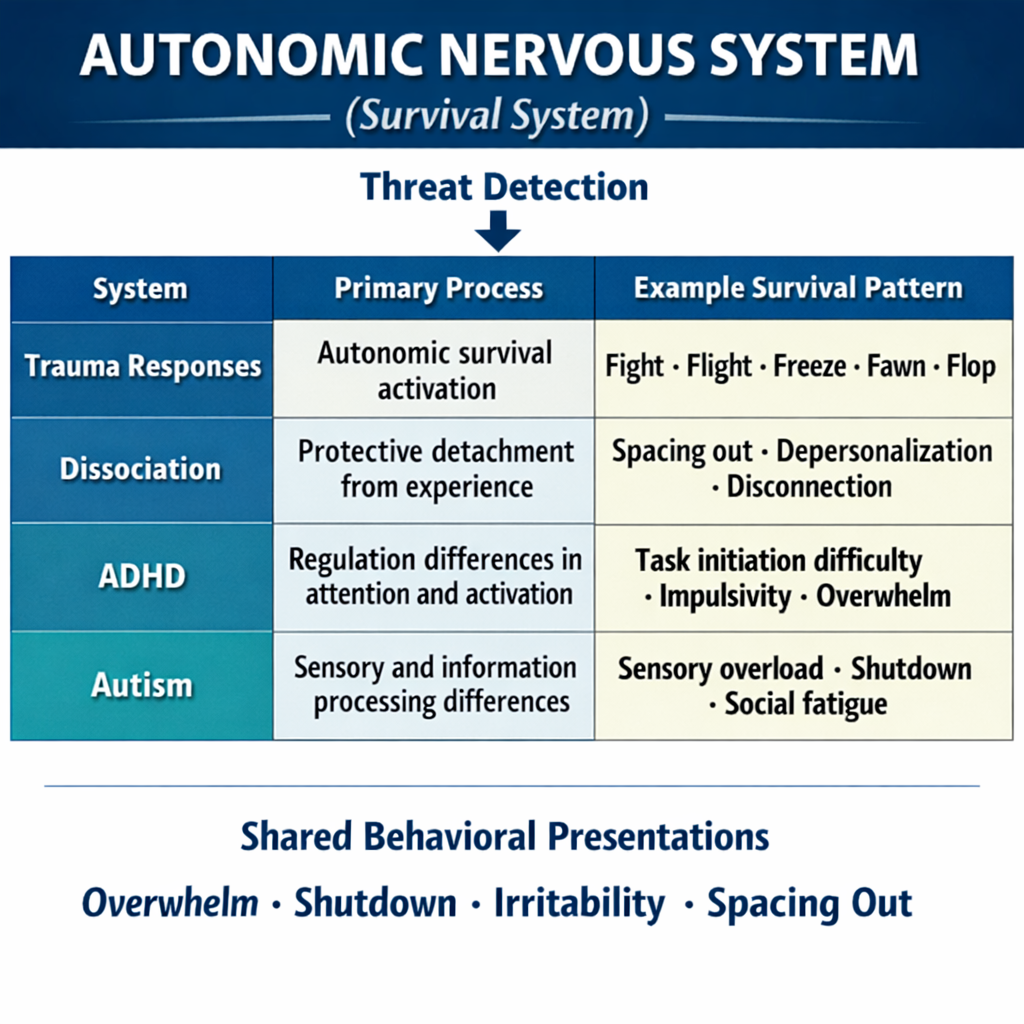
Most therapists today are familiar with the language of the nervous system. Fight, flight, freeze, fawn, and flop have become central to trauma-informed therapy and help clinicians recognize when behavior is driven by autonomic survival activation rather than conscious choice. What I like to call a reflex, something the body does to keep us alive.
This framework has transformed how therapists understand dysregulation. Instead of interpreting behavior as resistance or lack of motivation, clinicians increasingly recognize the role of physiological survival states. Yet many therapists eventually encounter a clinical puzzle, myself included.
A client cannot start tasks despite strong motivation. Another leaves social situations abruptly and describes it as "panic" or “too much.” Someone becomes irritable when overwhelmed and later reports exhaustion or shutdown. A client appears dissociated in session yet describes the experience as simply “spacing out.” These presentations raise an increasingly common clinical question:
The answer often involves an interaction between multiple nervous system processes. Trauma physiology may be present, yet the individual’s underlying neurotype can shape how that physiology emerges. When trauma responses intersect with neurodivergent processing styles, survival responses can appear in ways that are easily misunderstood.
Understanding this overlap has become an essential component of what I call neurodivergent trauma-informed care.
Trauma alters how the nervous system detects and responds to perceived threat. The autonomic nervous system organizes behavior along survival pathways, producing responses such as fight, flight, freeze, fawn, or flop when the brain detects cues of danger. But what happens when ADHD and Autistics neurology is different.
Neurodivergent individuals often experience the environment through nervous systems that already differ in several key areas:
These differences reflect variations in how the brain processes information. They shape how individuals filter sensory input, shift attention, manage cognitive load, and detect internal body signals.
When trauma experiences are layered onto these neurological patterns, survival responses can emerge in complex ways.
For example, sensory overload may activate the same survival physiology that interpersonal threat activates in others. This does not mean they have a trauma history they cannot remember. It means their body senses threats from sounds and lights. Executive functioning strain may move the nervous system toward immobilization. Attentional narrowing may resemble dissociation.
Without recognizing these intersections, therapists may misinterpret the signals the nervous system is communicating.
Another important layer involves the client’s neurotype.
Neurotypes such as ADHD and autism represent enduring patterns of neurological organization. These patterns influence how individuals regulate attention, process sensory information, shift cognitive focus, and recover from stress.
When a neurodivergent neurotype remains unrecognized, many lifelong experiences are interpreted through other frameworks. Chronic overwhelm may be labeled anxiety. Difficulty initiating tasks may be framed as avoidance or low motivation. Sensory sensitivity may be interpreted as emotional reactivity or chronic suicidality.
In therapy settings, these experiences can resemble trauma responses.
Persistent difficulty starting tasks may reflect ADHD-related executive functioning differences. Repeated shutdown in high-stimulation environments may signal sensory processing differences associated with autism. Deep absorption in specific interests may represent attentional style rather than dissociation.
When these patterns appear consistently across environments and developmental history, they may indicate an underlying neurodevelopmental profile rather than trauma physiology alone.
Many adults first encounter the concept of neurotype later in life. In these situations, trauma-informed therapy may uncover nervous system patterns that point toward previously unrecognized ADHD or autism.
Recognizing this possibility allows therapists to remain curious about the broader neurological context of a client’s experience.
One of the most common clinical challenges in this area involves diagnostic overshadowing.
Diagnostic overshadowing occurs when clinicians interpret symptoms entirely through one framework while overlooking the influence of another.
In practice, two patterns often appear.
In some cases, trauma responses are interpreted as neurodevelopmental traits. A freeze state may be labeled ADHD inattention. A collapse response may be viewed as depression or burnout. In other cases, neurodevelopmental traits are interpreted as trauma responses. Autistic monotropism may resemble dissociation. Sensory overload may be interpreted as anxiety or avoidance.
When this occurs, treatment can target the wrong regulatory system. The therapist may focus on cognitive insight or behavioral strategies that increase burnout while the underlying nervous system state remains unchanged. Shifting the clinical question helps address this issue. Rather than asking which diagnosis explains the behavior, clinicians can ask:
One nervous system state frequently misunderstood in neurodivergent clients is the freeze response.
Freeze occurs when the nervous system becomes caught between activation and shutdown. The body remains physiologically alert while the capacity for action becomes inhibited.
In therapy, freeze can resemble experiences commonly associated with ADHD:
From the outside, these experiences may appear as inattentiveness or lack of motivation.
Yet when freeze is present, the nervous system temporarily loses access to the pathways that support action. Executive functioning becomes difficult to access until regulation returns. In these moments, productivity strategies rarely resolve the issue. The nervous system must first regain physiological stability before executive functioning can reengage.
Recognizing freeze shifts the therapeutic focus toward regulation rather than performance. And just using regulation without addressing ADHD behavioral strategies only addresses half of the issue.
Another area of overlap involves the similarity between autistic shutdown and trauma-related collapse responses. Autistic individuals may enter shutdown states following prolonged sensory input, cognitive demand, or social effort. These states often include:
From the outside, shutdown can resemble depression, dissociation, or disengagement. Physiologically, however, the nervous system may be conserving energy after prolonged overload. This pattern aligns with the flop response in trauma physiology, in which the nervous system reduces activation after sustained stress.
Recognizing shutdown allows therapists to adjust expectations within sessions. Insight-oriented processing may be difficult while the nervous system remains in a recovery state. Stablization often requires reduced stimulation, pacing, and time. Understanding this response helps therapists avoid interpreting protective nervous system behavior as resistance. Shut down can be therapuetic and our client's form of coping.
Sensory input represents one of the most significant intersections between trauma and neurodivergence. For many individuals, trauma triggers involve interpersonal cues or situational reminders. For neurodivergent clients, sensory environments themselves can activate survival physiology.
Common triggers include:
When sensory input exceeds the nervous system’s processing capacity, the body may rapidly shift into survival activation. This activation may appear as agitation, withdrawal, shutdown, or dissociation depending on the individual’s nervous system pattern. Recognizing sensory triggers allows therapists to adjust the therapy environment and pacing in ways that supports stabilization. It teaches the client how to regulate, instead of using breathing while staying in a sensory dense enviroment.
Autistic cognition is often described through the framework of monotropism, a pattern in which attention becomes deeply focused on a limited number of stimuli. Monotropism supports sustained concentration, pattern recognition, and deep engagement with areas of interest.
Trauma can interact with this attentional style in ways that intensify distress. When threat cues become the focus of attention, the nervous system may repeatedly return to the same signals of danger. This process can create trauma attention loops in which perceived threat remains highly salient. Clinically, this may resemble rumination or hypervigilance.
Understanding monotropism helps therapists recognize that attentional patterns may be amplifying trauma physiology rather than reflecting cognitive distortion. Therapeutic work may focus on gently expanding attentional flexibility while respecting the strengths of focused cognition.
Another area that requires careful assessment involves the difference between dissociation and neurodivergent attentional states. Dissociation involves disruptions in the integration of awareness, memory, perception, or identity. It often emerges when the nervous system attempts to reduce overwhelming emotional intensity.
Several neurodivergent experiences may appear similar externally. ADHD inattention can involve shifting attention between competing stimuli. Autistic absorption can involve deep focus on a particular sensory input or topic. Dissociation can involve detachment or disconnection from present experience.
Although these states may appear similar during observation, their underlying mechanisms differ.
Structured assessments can assist clinicians in exploring these distinctions, including:
These tools support differential exploration of trauma physiology, attention regulation, and dissociative experience.
Effective trauma therapy with neurodivergent clients often involves adjustments in pacing and structure. Many trauma interventions rely on top-down processes such as cognitive insight, emotional labeling, and narrative processing. These approaches can be effective when the nervous system remains within a tolerable range of activation, are they in their window of tolerance.
Helpful adjustments may include:
These changes help the nervous system remain within a window where therapeutic engagement is possible.
Trauma-informed therapy continues to evolve as clinicians integrate findings from neuroscience, sensory processing research, and neurodevelopmental psychology. What is becoming increasingly clear is that trauma responses rarely occur in isolation. They interact with the individual’s neurological organization, sensory profile, attentional patterns, and developmental history.
When therapists view behavior through this expanded lens, many clinical puzzles begin to make sense. Agitation may reflect mobilization in response to overload. Withdrawal may signal nervous system protection following sensory saturation. Difficulty initiating tasks may involve freeze physiology, executive functioning strain, or both.
For some clients, trauma and neurodivergence coexist. For others, therapy may reveal patterns that point toward an underlying neurotype that had never been recognized, specifically with female Autistics. In these moments, the goal of therapy extends beyond symptom reduction. It includes helping clients understand how their nervous system works.
The nervous system has often been working diligently to protect the person long before therapy begins. Our work is to help it discover new pathways toward regulation, safety, and connection.
Frameworks such as fight, flight, freeze, fawn, and flop can help us organize what our clients are seeing in the nervous system, but they do not explain every presentation. Clients arrive with different neurotypes, sensory profiles, and developmental histories. Effective trauma-informed care begins with understanding how that person’s nervous system works, and then choosing interventions that fit their presentation rather than assuming a single model applies to everyone.

Rumball, F., Happé, F., & Grey, N. (2020). Experience of trauma and PTSD symptoms in autistic adults. Autism Research.
Kerns, C. M., Newschaffer, C. J., & Berkowitz, S. J. (2015). Traumatic childhood events and autism spectrum disorder. Journal of Autism and Developmental Disorders.
Botha, M., & Frost, D. M. (2020). Minority stress in autistic populations. Society and Mental Health.
Robertson, A. E., & Simmons, D. R. (2015). Sensory sensitivity and anxiety in autism. Autism.
Barkley, R. A. (2015). Executive functioning in ADHD. Annual Review of Clinical Psychology.
Murray, D., Lesser, M., & Lawson, W. (2005). Monotropism and autism. Autism.

For therapists, trauma-informed care is a primary focus in both training and treatment. This approach, characterized by sensitivity to trauma and its...
Trauma is a word that has been gaining more attention and importance in our society and in the therapy treatment world. We (therapists) all know what...

Neurodiversity-affirming therapy is emerging as a new approach to mental health care-one that flips the script on conventional therapy methods....